You realize that something has gone terribly wrong with your body. Your abdomen hurts from cramps when you don’t even eat anything. Your body has trouble going to the restroom; either way, it’s bad.
Your stomach is full of gas, sore, and unpredictable. But the question that far too many people struggle to answer for months, maybe years, is whether this condition is IBS or IBD.
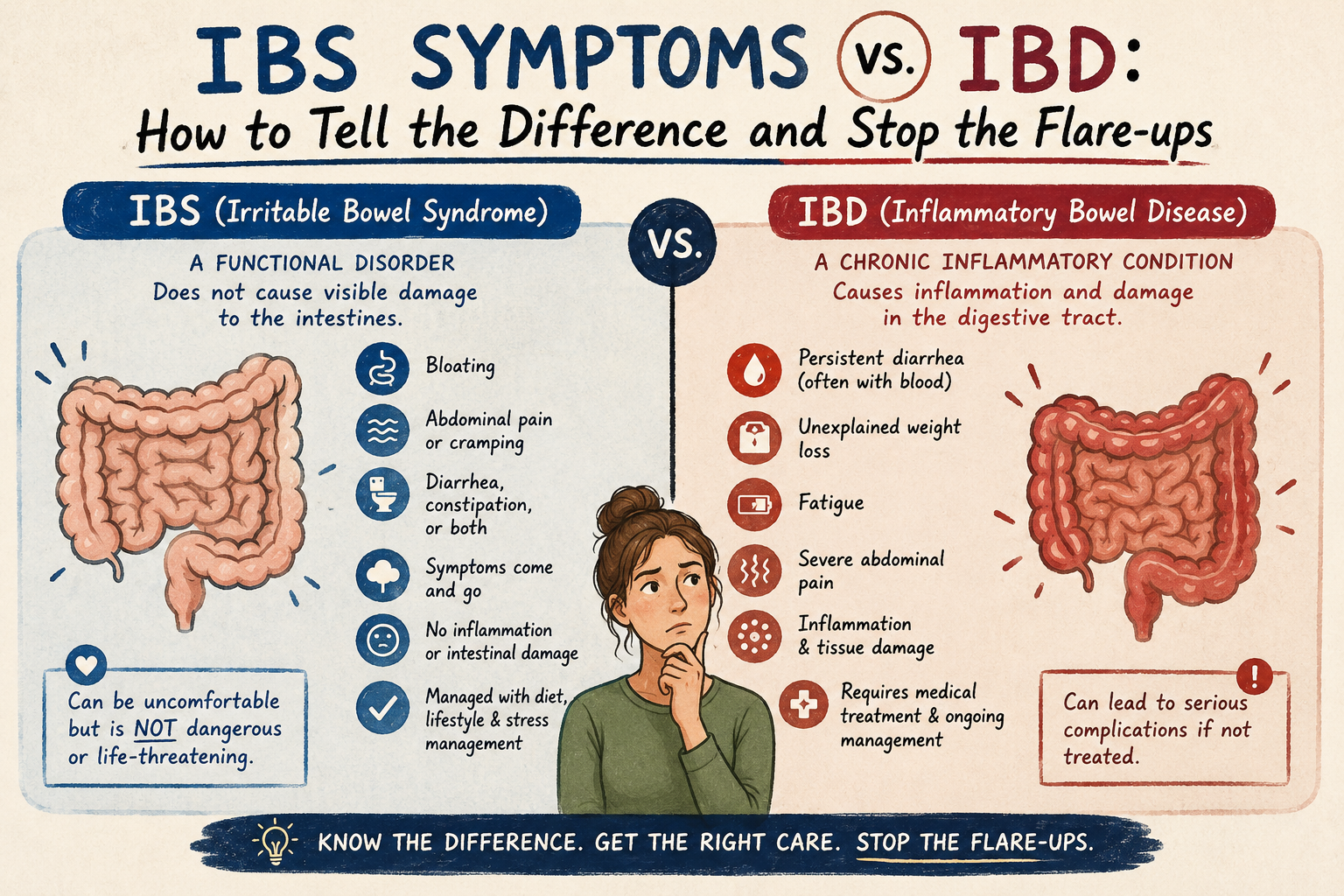
IBS (Irritable Bowel Syndrome) and IBD (Inflammatory Bowel Disease) are the two most often mistaken bowel disorders found within gastroenterology. Both share similar symptoms. Both use similar abbreviations. However, these diseases have fundamental differences that require completely different treatment approaches.
The Quick Answer: IBS is a functional disorder—your gut is miscommunicating with your brain, but there is nothing physically damaged. IBD is an autoimmune disease that results in actual, visible inflammation and structural damage to your gastrointestinal (GI) tract, confirmed by colonoscopy or biopsy. Treating one like the other could slow down your healing process, negatively affect your health outcome, and potentially cause irreversible damage due to prolonged inflammation.
In this article, you will learn exactly how to distinguish between the two conditions through specific symptoms and tests, as well as immediate actions you can take today to help stop a flare-up.
Irritable Bowel Syndrome (IBS) is a Functional Gastrointestinal Disorder. This means you have a problem with how your gut works; however, there is no obvious damage, inflammation, or structural abnormality.
To make an official diagnosis of IBS, doctors rely upon the Rome IV criteria, which requires recurring abdominal pain for at least 1 day/week associated with changes in either bowel frequency and/or consistency for a minimum of 3 months.
In the U.S., an estimated 25-45 million adults suffer from IBS, representing approximately 10-15% of all adults globally, as reported by the American College of Gastroenterology. It is the most commonly diagnosed medical condition among gastroenterologists worldwide.
There are 3 primary types of IBS:
IBS-C (Constipation-dominant): Infrequent, hard stools; straining; severe bloating.
IBS-D (Diarrhoea-dominant): Loose stools; urgency; frequent bathroom trips.
IBS-M (Mixed): Alternates between constipation and diarrhoea.
The primary issue behind IBS is a dysfunction of the Gut-Brain Axis (GBA)—the bidirectional communication network between your digestive tract and your brain. When the GBA misfires, it results in visceral hypersensitivity, altered gut motility, and microbiome disruption. Common triggers include stress, anxiety, and specific food intolerances.
Inflammatory Bowel Disease (IBD) is an autoimmune disorder where the body’s immune system mistakes normal GI tissue for a threat, attacking and inflaming the area long-term. As opposed to IBS, IBD results in physical changes to the tissues of the GI tract that are observable and verifiable via colonoscopy, biopsy, and imaging.
IBD encompasses two separate medical conditions:
Crohn’s Disease: Can affect any part of the GI tract (from mouth to anus). It causes deep, patchy inflammation through all layers of the bowel wall and is associated with fistulas, abscesses, and bowel narrowing.
Ulcerative Colitis (UC): Confined strictly to the colon and rectum. It causes continuous surface inflammation and ulcers along the colon lining and almost always involves rectal bleeding.
According to the Crohn’s & Colitis Foundation, over 3 million people have been diagnosed with IBD. If left uncontrolled, misdiagnosed, or untreated, IBD will continue to cause progressive structural damage over time.
Untreated IBD can lead to severe consequences, including:
Permanent scarring and narrowing of the bowel (strictures)
Abnormal channels connecting various organs (fistulas)
Severe anaemia due to prolonged internal bleeding
A significantly higher risk of developing colorectal cancer
Managing IBD as one would manage IBS is not only ineffective, but medically hazardous.
Both conditions cause chronic abdominal pain, cramps, diarrhoea, and bowel urgency. However, identifying condition-specific “red flags” dictates correct medical intervention.
| Feature | IBS (Irritable Bowel Syndrome) | IBD (Inflammatory Bowel Disease) |
| Disease Type | Functional disorder | Autoimmune / Structural disease |
| Visible GI Damage | None | Yes (confirmed by colonoscopy) |
| Bleeding | Never | Common (especially in UC) |
| Fever | No | Yes (during active flares) |
| Weight Loss | Rare | Common |
| Primary Triggers | Stress, diet, anxiety | Immune response (not diet alone) |
| Primary Treatment | Diet, lifestyle, stress management | Medication, biologics, surgery |
IBS: Lower abdomen. Often relieved after a bowel movement; triggered by stress or eating.
Crohn’s disease: Lower right side. Persistent, unrelieved by bowel movements; may worsen after eating.
Ulcerative colitis: Lower left side. Cramping before and during bowel movements, almost always accompanied by rectal bleeding.
If you experience any of the following, this points to IBD, not IBS. Seek medical attention promptly.
Rectal bleeding or blood in your stool
Unexplained weight loss
Persistent fever
Chronic fatigue and anaemia
Symptoms that wake you from sleep
Diarrhoea that does not improve with dietary changes
The diagnostic pathways are fundamentally different.
IBS Diagnosis (Diagnosis by Exclusion):
Symptoms meet Rome IV criteria.
Blood tests, stool tests, and imaging return normal results.
Colonoscopy shows healthy tissue with no inflammation.
Normal Fecal Calprotectin levels.
IBD Diagnosis (Diagnosis by Confirmation):
Colonoscopy with biopsy reveals active inflammation or ulcers.
Elevated Fecal Calprotectin (a key stool biomarker for intestinal inflammation).
Elevated CRP (C-reactive protein) blood test.
MRI or CT scan reveals bowel thickening or fistulas.
Anaemia or low albumin on blood work.
Do not wait for a routine appointment if you experience:
Rectal bleeding or blood in your stool, at any amount.
Unintentional weight loss of more than 5% of your body weight.
Fever above 38°C (100.4°F) alongside gut symptoms.
Symptoms that wake you from sleep at night.
Severe abdominal pain that does not resolve within a few hours.
Family history of IBD, Crohn’s disease, or colorectal cancer.
Lifestyle and dietary interventions can effectively treat IBS flare-ups. In contrast, IBD flare-ups require medical oversight—lifestyle changes alone will not provide sufficient relief and may exacerbate tissue damage.
The Low-FODMAP Diet: Removes fermentable carbohydrates that cause bloating and gas. Symptoms improve in ~76% of IBS patients.
Probiotics: Strains like Lactobacillus and Bifidobacterium help restore microbiome balance (best for IBS-D/IBS-M).
Cognitive Behavioral Therapy (CBT): Targets the gut-brain connection, reducing symptoms by up to 60%.
Soluble Fiber Adjustment: Psyllium husk eases both diarrhoea and constipation, whereas insoluble fiber (bran) can trigger symptoms.
Stress Reduction: Mindfulness, yoga, and diaphragmatic breathing reduce central nervous system stress on the gut.
Anti-inflammatory medications: 5-ASA compounds (e.g., Mesalamine) as first-line UC treatment.
Corticosteroids: Prednisone for short-term acute inflammation suppression.
Biologics: TNF inhibitors (e.g., Infliximab, Adalimumab) for moderate-to-severe IBD.
Immunomodulators: Azathioprine or Methotrexate to reduce immune activity.
Consistent Sleep: Poor sleep worsens systemic inflammation and gut motility.
Moderate Exercise: 30 minutes of daily low-impact activity lowers flare-up frequency.
Trigger Avoidance: Eliminating alcohol, excess caffeine, and ultra-processed foods.
The three critical takeaways to remember:
IBS never causes structural damage to your GI tract; IBD causes cumulative, visible damage unless medically treated.
Rectal bleeding, fever, and unexplained weight loss are never caused by IBS. If you have these symptoms, assume IBD until a doctor proves otherwise.
IBS is managed through diet and lifestyle; IBD requires targeted medical prescriptions.
If your symptoms continue or worsen, do not try to self-manage. At Longeny, we go beyond standard diagnostics. Our team utilizes India’s most advanced technology for analyzing your microbiome via a comprehensive gut microbiome test, combined with personalized doctor access and an online nutritionist consultation.
Whether you are battling chronic IBS symptoms or suspect early-stage IBD, Longeny’s 90-Day Gut Repair Plan provides a structured, biological-first system to heal your gut. Quit guessing. Start measuring.
Q1: Will IBS turn into IBD?
No. IBS does not develop into IBD. IBS is a functional disorder that affects how the bowel works, while IBD is an inflammatory disease that damages the digestive tract. However, persistent or changing symptoms should always be assessed by a doctor.
Q2: Are IBS and IBD the same condition?
No. Although they can share symptoms such as abdominal pain and changes in bowel habits, they are very different conditions. IBD causes ongoing inflammation that can damage the intestine, whereas IBS does not cause inflammation or permanent bowel injury.
Q3: How does an IBD flare compare to an IBS episode?
An IBD flare often involves intestinal inflammation and may include bloody stools, fever, weight loss, fatigue, and raised inflammatory markers. An IBS episode usually causes abdominal pain, bloating, constipation, diarrhea, or both, but does not cause intestinal damage or bleeding.
Q4: Can both IBS and IBD occur at the same time?
Yes. Some people with well controlled IBD continue to experience IBS like symptoms such as bloating or abdominal pain even when inflammation is no longer active. A medical evaluation can help determine whether symptoms are due to ongoing inflammation or altered gut function.
Anil K.C. is the founder of LONGENY, a precision health platform focused on extending healthspan, and longevity, through science-backed diagnostics, nutrition, and personalized care. A serial entrepreneur and host of the Brighter100 podcast, he translates complex longevity science into clear, actionable insights.
